Risk of cardiovascular disease decreases over time in psoriatic arthritis but not in spondylarthritis: meta-analysis of longitudinal studies
Introduction
Cardiovascular (CV) and metabolic diseases represent the most frequent comorbidities in patients with PsA and axSpA, with a prevalence reaching 12% in SpA (Zhao et al.) and 19% in PsA (Gupta et al.).
Increased risk may be related to chronic inflammation, treatments (NSAIDs, steroids), and other risk factors (e.g., hypertension).
Meta-analysis of controlled observational studies assessed CVD risk over time in SpA and PsA patients, with a secondary objective to evaluate if new therapies and a treat-to-target approach reduced such risk.
Methods
Systematic literature review (SLR) from 1990 to December 2021.
Main outcome: composite occurrence of CVD, including ischaemic heart disease (IHD), stroke, and CV-related death.
Studies included had a follow-up period of at least 5 years.
Prespecified adjustments: age, gender, CV risk factors, and comorbidities.
Random-effects model and inverse variance method used to estimate pooled hazard ratios (HRs) with 95% confidence intervals (CIs).
Results
24 manuscripts included: 16 on SpA (113,827 cases) and 10 on PsA (93,118 cases), with 2 studies covering both.
SpA patients had an increased CVD incidence compared to the general population (pooled HR 1.45; 95% CI 1.22–1.72), also for individual CVS events.
PsA patients showed increased CVD incidence compared to the general population (pooled HR 1.28; 95% CI 1.15–1.43), excluding death.
Incident CVD rates in PsA patients decreased over time.
bioDMARD therapies were associated with reduced CVD risk, particularly in SpA.
NSAID effects on CVD risk were inconsistent, with some studies indicating increased risk from recent use, while others showed decreased overall incidence.
H. Gouze, P. Aegerter, Y. Gouyette, et al., Rheumatology, 16 February 2024
A disease-associated gene desert directs macrophage inflammation through ETS2
Examination of H3K27ac chromatin immunoprecipitation–sequencing (ChIP–seq) data, which marks active enhancers and promoters, a monocyte/macrophage-specific enhancer has been identified within the locus
Using promoter-capture Hi-C and expression quantitative locus (eQTL) data from human monocytes (Methods), the disease-associated locus physically was shown to interact with the promoter of ETS2 and that the risk haplotype correlates with higher ETS2 expression
Used a CRISPR–Cas9-based loss-of-function approach and designed two gRNAs targeting different ETS2 exons to assess impact of reducing expression of ETS2
Transfected non-activated macrophages with ETS2 mRNA and examined the impact of overexpression of ETS2exposure after stimulation with low dose lipopolysaccharide
Spatial transcriptomics and bulk RNA-seq data from diseased human tissues was used to examine ETS2 gene expression
Used MEK ½ inhibitors, which downregulate ETS-2 target genes, to assess anti-inflammatory activity in cultured macrophages and intestinal biopsies
Results
Single nucleotide polymorphism, rs2836882, in EST2 enhancer had strong EST2 gene expression-modulating effect
SNPs associated with ankylosing spondylitis were enriched in ETS2-target genes.
Targeting ETS2 markedly reduced pro-inflammatory cytokine production (IL-6, IL-8 and IL-1β), phagocytosis and oxidative burst, expression of inflammatory cytokines chemokines, secreted effector molecules, cell surface receptors, and signalling molecules
Overexpression of ETS2 resulted in dose-dependent macrophage activation of all inflammatory pathways
Differential expression of ETS2-regulated genes was observed in macrophages from IBD patients stratified by rs2836882 genotype
Transcriptional footprint of ETS2 was detectable in affected tissues from multiple chr21q22-associated diseases
MEK inhibition reduced inflammatory cytokine release to similar levels as infliximab
Several classes of drugs phenocopy ETS2 disruption, including JAK inhibitors.
Collectively, these data identify an essential role for ETS2 in macrophage inflammatory responses
C. T. Stankey, C. Bourges, L. M. Haag, et al., Nature, 05 June 2024
Incidence of Uveitis in Patients With Axial Spondylarthritis Treated With Biologics or Targeted Synthetics: A Systematic Review and Network Meta-Analysis
EULAR 2022 and ACR2019 treatment recommendations recommend TNFi as preferred DMARD when axSpA patients have concomitant AAU (Ramiro et al.) (Ward et al.)
Network meta-analysis demonstrated lower risk of AAU with TNFi versus IL17i bioDMARD in axSpA (Roche et al.)
This SLR was aimed at updating the analyses to include data from upadacitinib and bimekizumab RCTs
Methods
SLR used MEDLINE and EMBASE and was run to December 2023
Included all placebo-controlled RCTs of TNFi, IL17i, and JAKi in AS and nr-axSpA plus their open label extensions
Primary outcome was AAU events (new onset and relapse)
Pooled estimates of the relative risk of AAU between each treatment arm and placebo were compared using Network Meta-Analysis (NMA) and expressed as incidence rate ratios (IRRs) with 95% CIs
Results
44 placebo-controlled RCTs were included
26 studies reported on AAU during the trial period in their safety analyses.
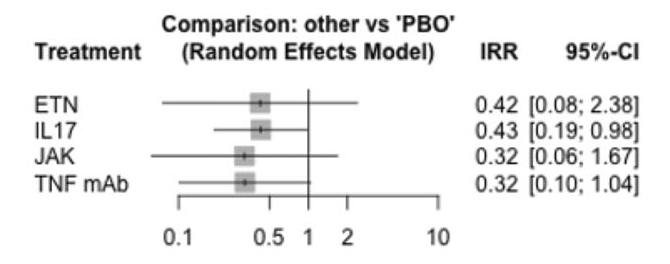
IRs of AAU per 100 patient-years were 4.1[95% CI 0–8.5] for TNFi mAbs, 5.4 [95% CI 0–16.0] for etanercept, 2.8 [95% CI 1.6–4.1] for IL-17i, and 1.5 [95% CI 0.0–3.0] for JAKi.
In the pooled placebo group, IRs were 10.8 [95% CI 7.4–14.1] per 100 person-years.
IL-17i was the only group to demonstrate a statistically significant lower IRR compared to placebo. Tap/click on the image for a larger view
Katie Bechman, Zijing Yang, Maryam Adas, et al; ARTHRITIS RHEUMATOLOGY, 20 December 2023
Association of nociplastic and neuropathic pain components with the presence of residual symptoms in patients with axial spondyloarthritis receiving biological disease-modifying antirheumatic drugs
Introduction
It is uncommon to see complete resolution of spinal symptoms in patients with axSpA receiving bioDMARD or targeted synthetic DMARD
This could be an example of nociceptive pain i.e. stimulation of afferent pain fibres by proinflammatory mediators.
It could also reflect abnormal central and/or peripheral pain processing unrelated to joint inflammation or structural damage, or any abnormality of neural tissue (neuropathic pain), this being termed nociplastic pain
The International Association for the Study of Pain has standardized categorization of pian into 3 descriptors based on mechanistic considerations: nociceptive, neuropathic, nociplastic (Kosek et al).
There is little understanding of the etiology of residual pain in axSpA, and especially the role of neuropathic and nociplastic pain.
Methods
78 patients about to start a bioDMARD for axSpA in the German Spondyloarthritis Inception Cohort (GESPIC) were prospectively followed
The Widespread Pain Index (WPI) (Wolfe et al) was used to assess nociplastic pain and neuropathic pain was assessed using the PainDETECT (PD) questionnaire (Freynhagen et al).
Residual symptoms were defined as a Bath AS Disease Activity (BASDAI) >4 and/or AS Disease Activity Score (ASDAS) >2.1
Multivariate regression assessed the association between the WPI/PD and the BASDAI/ASDAS thresholds.
Results
Most patients received TNF inhibitor bioDMARD
According to the WPI, a possible nociplastic component (WPI 3–6) was detected in 41% patients and a likely component (>6) in 5% patients
Only 8% had a possible (PD 13–18) and 1% patient a likely (>18) neuropathic component according to the PD score
Of 31% with residual symptoms (ASDAS>2.1), 79.2% showed either a possible or likely nociplastic component and 20.8% patients showed a possible or likely neuropathic component.
Both WPI and PD were shown to be independently associated with ASDAS and BASDAI
WPI was shown to be independently associated with ASDAS>2.1 and BASDAI >4
Fares Al Mohamad, Valeria Rios Rodriguez, Hildrun Haibel, et al; RMD Open 2024
Comparison of the effect of treatment with NSAIDs added to anti-TNF therapy versus anti-TNF therapy alone on the progression of structural damage in the spine over 2 years in patients with radiographic axial spondyloarthritis from the randomised-controlled CONSUL trial
Introduction
Predictors of structural damage in the spine in axSpA include pre-existing ankylosis/syndesmophytes, high disease activity, and spinal inflammation on MRI.
A previous study suggested that celecoxib may prevent progression of structural damage, especially in patients with elevated ESR/CRP (Wanders et al), but a similar study evaluating diclofenac (Sieper et al) did not support this effect of NSAID therapy.
Observational studies have reported that TNF inhibitors may prevent structural progression (Sepriano et al).
It is unclear if adding NSAID therapy to TNF inhibition retards radiographic progression in radiographic axSpA patients at high risk (either presence of syndesmophytes and/or elevated CRP).
Methods
Study design included a 12-week ‘run-in phase’ of golimumab 50 mg for all subjects and then responders (BASDAI decrease of ≥2 (0-10 scale)) were randomized 1:1 to golimumab plus celecoxib (GOL/CEL) versus golimumab (GOL) alone for 96 weeks.
Primary endpoint was change in mSASSS at 2 years.
A difference of 1.5mSASSS units between groups was used for sample size calculations (worsening of 1.7 and 0.2 mSASSS units in GOL and GOL/CEL groups, respectively). 38 were deemed necessary for 80% power.
Results
Of 109 patients that were randomized, 97 (89%) completed the study at week 108.
Prior treatment with bDMARDs in 31.5% in the GOL/CEL group vs 16.4% in the GOL group.
In the GOL group, 23 (42.6%) patients received NSAIDs at least once.
Mean mSASSS change over 2 years was numerically higher in the GOL group (1.7; 95% CI 0.8 to 2.6) vs the GOL/CEL group (1.1; 95% CI 0.4 to 1.8) (p=0.79).
New syndesmophytes in 25% GOL vs 11% GOL/CEL (p=0.12)
All the sensitivity analyses numerically favored the GOL/CEL group
No significant difference in disease activity or adverse events between the groups
Ann Rheum Dis 2024
Common incidental findings on sacroiliac joint MRI: Added value of MRI-based synthetic CT
Introduction
A novel technique based on MRI for visualizing osseous structures is synthetic CT (sCT), a deep learning-based multiparametric MRI technique that permits the creation of radiograph-like and CT-like images without ionizing radiation.
It has been shown to outperform T1-weighted MRI-images for detection of erosions, sclerosis and ankylosis of the SI joint in patients with axSpA (Jans, Chen et al).
The aim of this study was to determine the prevalence of incidental findings demonstrated on MRI of the SI joints in patients clinically suspected of axSpA and to examine the added value of the additional sCT.
Methods
Retrospective study of 214 patients clinically suspected of axSpA who underwent a conventional diagnostic MRI with STIR and T1W sequences
For sCT reconstruction an additional axial three-dimensional T1-weighted radio-frequency-spoiled multiple gradient echo (3DT1MGE) sequence was scanned
Two readers independently determined: (1) The lesion is only visible on sCT, (2) the lesion is visible on sCT and the conventional sequence (T1 TSE or T2 STIR), (3) the lesion is only visible on the conventional sequence (T1 TSE or T2 STIR).
Results
In 44.7% of patients sacroiliitis was present.
187 (89.0 %) of all patients MRI showed one or more incidental findings.
Degeneration of SIJ was most frequent (66.6%)
The most frequent incidental findings outside the sacroiliac joint were facet joint degeneration (29.0%), disc degeneration (25.2%), enostosis (19.5%) and lumbosacral transitional vertebrae (14.3%).
Synthetic CT was found to be problem solving or necessary for diagnosis in 543 (68.9%) of these lesions. 42.1% of lesions were not visible on conventional MRI (T1 TSE and STIR).
EJRad, vol158, 110651, jan2023
In vitro profiling of rheumatic-disease-evaluated JAK inhibitors demonstrate differences in JAK isoform selectivity between different types of inhibitors
Introduction
JAK inhibitor selectivity forms the basis for understanding differences in efficacy and safety of JAKinibs. Filgotinib and upadacitinib are considered to be more JAK1 selective.
Evaluation has been hampered by the lack of comprehensive JAKi head-to-head studies and assay-to-assay variation in individual studies.
Methods
10 JAKi (5 globally approved for rheumatic diseases (pan-JAKi tofacitinib, baricitinib, peficitinib and JAK1i filgotinib and upadacitinib)) were analyzed for JAK-isoform selectivity by assaying:
inhibition of catalytic activity
binding to kinase and regulatory pseudokinase domains
inhibition of cytokine signaling in peripheral blood of healthy volunteers
inhibition of STAT phosphorylation at clinically relevant JAKi concentrations in PBMC of RA patients and healthy donors.
Results
In vitro inhibition of kinase activity, pan-JAKi (tofacitinib, baricitinib) targeted JAK1-2 with high potency and comparably with JAK1 selective agents. Filgotinib and upadacitinib also targeted JAK2 (2-fold selectivity for JAK1). TYK2 and JAK1 was targeted by deucravacitinib and beprocitinib (also JAK1).
In human leukocytes, JAKi predominantly inhibited JAK1-dependent cytokines
IL-2, IL-6, and interferons. Inhibition of these cytokines was more pronounced in RA cells compared to healthy controls.
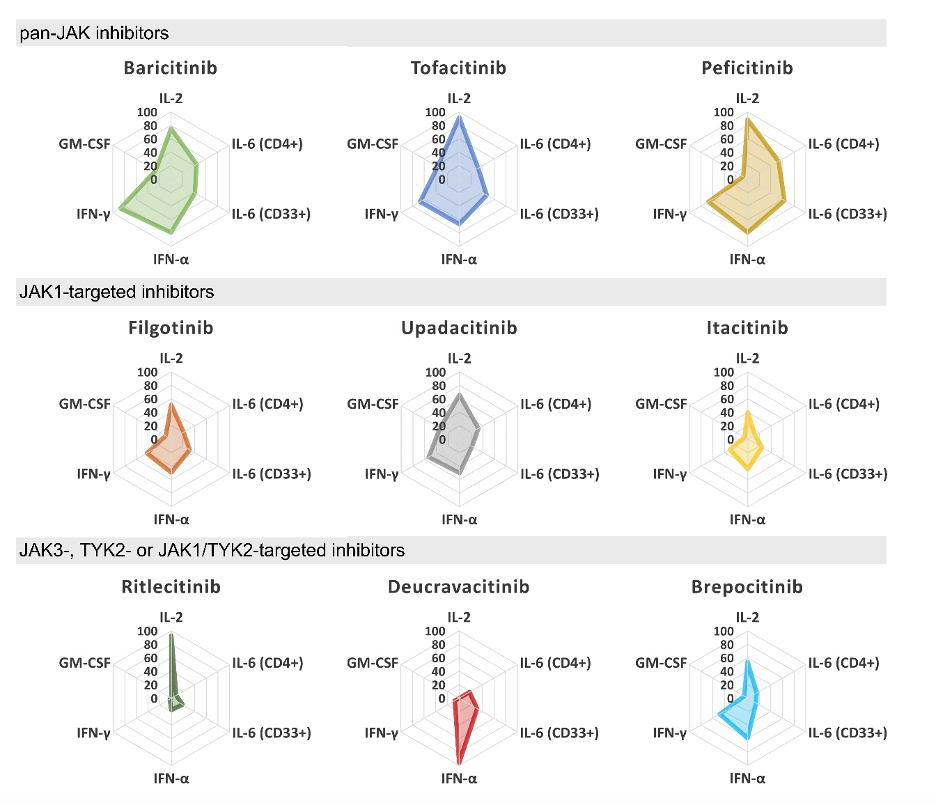
Pan-JAK and JAK1-targeted JAKi showed similar inhibition profiles at clinically applied dose in PBMCs of RA but the inhibition levels varied (Figure). Tap/click on the image for a larger view Figure.Cytokine inhibition profiles of JAKi in immune cells of RA patients. Inhibition
percentages of cytokine-induced STAT phosphorylation for clinically relevant concentrations
of JAKi. IL-2 and IFN-α inhibition was measured in CD4+ T cells, and IFN-γ and GM-CSF
inhibition in CD33+ monocytes.
Arthritis Rheumatol. 2023 May 3. doi: 10.1002/art.42547
Impact of NSAIDs on 8-year cumulative incidence of major cardiovascular events in patients with ankylosing spondylitis: a nationwide study
Introduction
Cardiovascular risk factors are frequent in patients with axial spondyloarthritis (axSpA)
There is an increased frequency of major cardiovascular events (MACE) in patients with axSpA as highlighted in a recent meta-analysis (Kim JH, Choi IA).
Clinicians are therefore concerned that the use of NSAIDS in axSpA may further increase the risk of MACE.
The impact of other therapeutics is unclear although tumor necrosis factor inhibitors (TNFi) have been shown to reduce subclinical atherosclerosis (Atzeni et al).
Methods
These investigators studied the occurrence of MACE in the French national medical administrative database SNDS
Ankylosing spondylitis (AS) was identified by the M45 ICD-10 code and the long-term illness designation #27 was used as a marker of active SpA
All French patients newly receiving Long Term Illness benefits for AS from 2010 to 2013 were included. The final follow-up date was 31 December 2018.
Competitive risk analysis using propensity score and inverse weighting was performed to
calculate cumulative incidence of MACE and determine subhazard ratios (SHRs) for the various treatments of interest.
Results
A total of 22 929 individual patients were included.
The 8-year cumulative incidence of MACEs, stroke, and MI were 1.81% (1.61–2.05), 0.97% (0.83–1.14), and 0.85% (0.71–1.04), respectively.
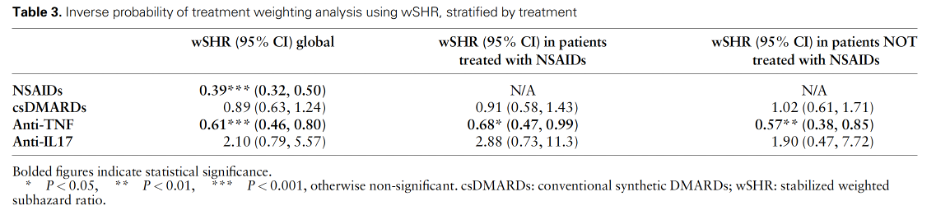
NSAIDs and TNFi drugs were associated with a lower risk of MACEs.
Interleukin-17 inhibitor (IL17i) therapy was not related to the risk of MACE. Tap/click on the image for a larger view
Efficacy and safety of upadacitinib in patients with active psoriatic arthritis and axial involvement: results from two phase 3 studies
Introduction
Axial inflammation in psoriatic arthritis (axPsA) is an important phenotype that may affect as many as 70% of patients with PsA and is associated with higher disease activity and impairment of quality of life.
AxPsA may respond differently to therapeutics versus peripheral PsA
This post-hoc analysis assessed the impact of upadacitinib in patients with active PsA and axial involvement in the SELECT-PsA trials.
Methods
Patients with inadequate response or intolerance to ≥1 conventional synthetic DMARD (SELECT PsA-1) or ≥1 bio-DMARD (SELECT PsA-2) were randomized to upadacitinib 15mg or 30mg or placebo daily or adalimumab 40mg every other week for 24 weeks.
At 24 weeks placebo patients switched to upadacitinib 15mg or 30mg daily to week 56
Axial involvement was determined by investigator judgement (yes or no) based on the totality of available clinical information, lab investigations and imaging, if available.
Patients had to have BASDAI >4 and BASDAI item 2 (overall neck, back, or hip pain) >4 at baseline.
Efficacy outcomes included BASDAI, modified BASDAI excluding item 3 (peripheral pain), BASDAI 50 response, ASDAS, ASDAS <2.1 and <1.3, ASDAS MI response.
Results
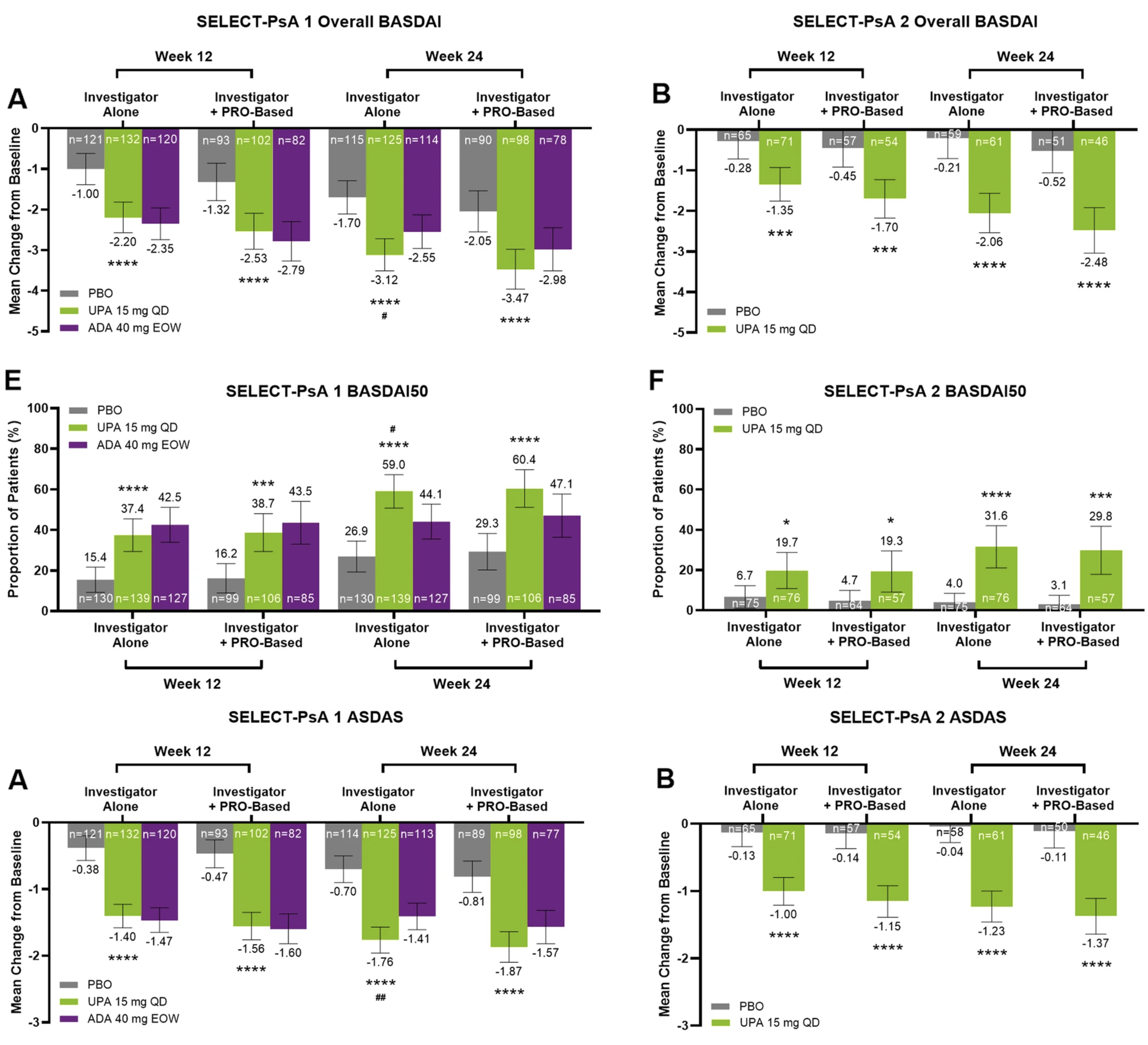
30.9% of PsA patients in SELECT-PsA 1 and 35.7% in SELECT-PsA 2 (bDMARD-IR) were defined as having axial involvement based on investigator judgement alone.
BASDAI and ASDAS score improvements were greater with upadacitinib 15 mg versus placebo at weeks 12 and 24 in both studies and according to both criteria used to define axial involvement. Tap/click on the image for a larger view
PsA patients treated with upadacitinib 15 mg showed consistent numerically higher responses than adalimumab across the efficacy endpoints regardless of the criteria used to define axial involvement.
Arthritis Research & Therapy volume 25, Article number: 56 (2023), Baraliakos et al
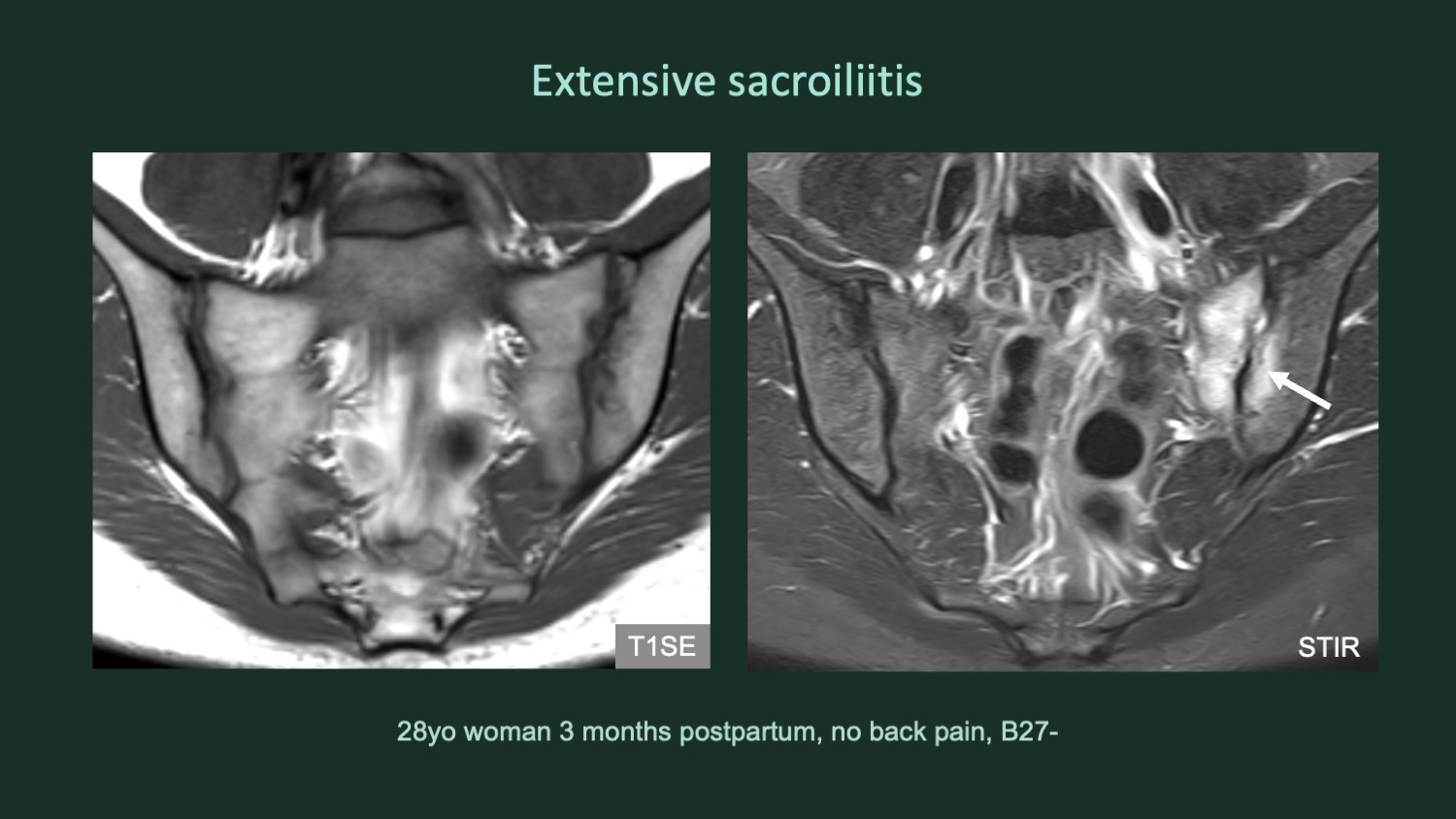
Evolution of MRI Lesions at the SIJ During and After Pregnancy by Serial Magnetic Resonance Imaging From Gestational Week Twenty to Twelve Months Postpartum
Introduction
It has been known for some time that bone marrow edema (BME) may be observed in the sacroiliac joints (SIJ) on MRI in postpartum women which is not necessarily associated with low back or buttock pain.
It is thought that postpartum BME is related to birth trauma but there have been no prospective studies evaluating SIJ abnormalities on MRI during healthy pregnancy to determine when BME first becomes evident.
There is little information on the precise localization of the BME and the degree of its persistence during propsective follow up post-partum.
Systematic assessment of structural lesions in the SIJ on MRI and their evolution during and after pregnancy are very sparse.
Methods
MRI was performed on 50 consecutive healthy pregnant women attending antenatal care at gestational weeks 20 and 32 and at 3, 6, and 12 months postpartum.
MRI was also performed on an additional 53 healthy postpartum women at 3, 6, and 12 months
MRI scans in the postpartum period were assessed in both the oblique coronal and semiaxial orientations to permit precise localization of BME
BME and structural MRI lesions in the SIJ were quantified using the Spondyloarthritis Research Consortium of Canada (SPARCC) methods
MRI lesions were also assessed using the CARE ARTHRITIS web-based interface according to the 2021 ASAS definitions for definite BME (present in ≥4 SIJ quadrants), erosion (present in ≥3 SIJ quadrants), and fat lesion (present in ≥5 SIJ quadrants) (Maksymowych et al. Rheumatol 2021; 60: 4778-89).
Detailed clinical evaluation for axSpA was performed at 12 months.
Results
BME was already evident at 20 weeks (62%) and 32 weeks (73%) of pregnancy
Prevalence and extent of BME peaked at 3 months postpartum, where 68.7% and 41.0% of women had a SPARCC BME score of ≥1 or ≥4, respectively.
At 12 months postpartum, SPARCC BME scores of ≥1 and ≥4 were reported in 53.5% and 19.7% of women, respectively.
At 12 months postpartum, sacroiliitis according to the 2021 ASAS definition for definite BME was found in 21%.
BME was most frequently observed in the anteromedial cartilaginous portion of the ilium and sacrum.
Definite erosion according to the 2021 ASAS definition was rare (2.8%).
Image provided by courtesy of Dr. Ulrich Weber
Arthritis Rheumatology 2023 Jan 26 Online Kiil RM, et al.